
The history of prosthetics designed to aid individuals with upper-limb differences is rich with innovation, yet significant challenges persist. For children, these challenges are amplified due to rapid growth, making access to appropriate prosthetic devices particularly crucial for their psychosocial development. Unfortunately, devices that offer both cosmetic appeal and functional utility are often beyond reach for children due to prohibitive costs, restrictive insurance policies, limited medical availability, and concerns about durability and complex operation. These barriers have spurred a global grassroots movement seeking to provide viable, affordable solutions for millions worldwide living with limb differences. The groundbreaking application of 3D printing technology, enabling customized and user-specific hardware, has paved the way for open-source, Do-It-Yourself (DIY) production of assistive devices, creating a profound global impact, especially for families with limited resources. This article delves into the latest research and advancements in 3D printed prosthetics spearheaded by maker communities and non-profit organizations. We will also examine a compelling case study that explores technological development alongside effective training methodologies. Furthermore, we will contextualize these innovative design efforts within the medical regulatory landscape of the United States, highlighting emerging clinical studies designed to quantify the impact of such devices on the quality of life for users.
Keywords: 3d Printing Prosthetics, prosthetics, upper limb prosthetics, pediatric prosthetics, assistive technology, open source, DIY, maker movement, quality of life, gamification
1. The Evolution and Enduring Need for Prosthetic Innovation
The concept of prosthetic limbs stretches back to ancient civilizations, with evidence from Egypt and Rome demonstrating early attempts at replacing missing limbs [1, 2]. Prosthetic design continued its evolution through the ages, reaching a turning point in the late 19th century with the development of the Hanger Limb by John Hanger, born out of the needs arising from the American Civil War [3]. This invention marked the beginning of modern prosthetic design. Medical progress since then has dramatically reduced limb loss resulting from traumatic injuries [4, 5]. However, in 2005, it was estimated that 1.6 million individuals in the United States were living with limb differences [6], with approximately 541,000 experiencing some degree of upper-limb loss [6]. Projections indicate this number could double by 2050 [6], underscoring the continued and growing need for effective prosthetic solutions. Trauma remains the leading cause of upper-limb amputation, particularly among males [7], while a concerning rise in dysvascular-related amputations in adults is also observed. Congenital limb differences and pediatric amputations represent a significant portion of the overall population with limb loss [9, 10, 11], monitored globally by organizations such as the International Clearinghouse for Birth Defects Surveillance and Research [8].
In the United States alone, over 32,500 children have undergone major pediatric amputations [10]. The Centers for Disease Control and Prevention estimates that around 1,500 children are born with upper-limb reductions each year, affecting approximately 4 out of every 10,000 live births [12]. Internationally, the prevalence of limb reductions varies, ranging from 7.8 per 10,000 births in France [9, 13] to 30.4 per 10,000 in Scotland [14], highlighting a global spectrum of need. Despite advancements in prosthetic technology, access barriers and user preferences contribute to limited device utilization rates among amputees.
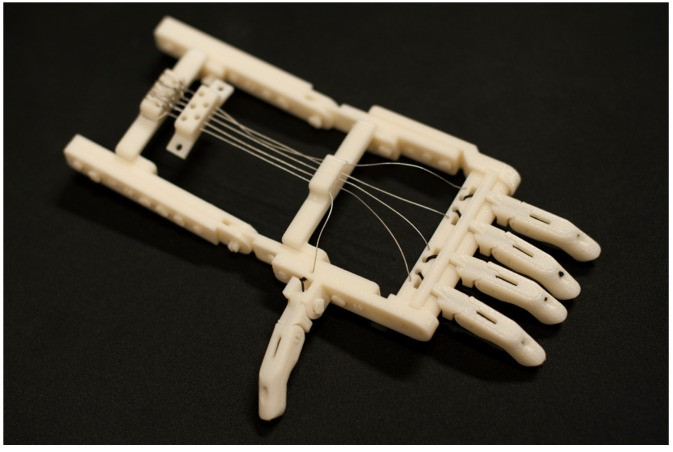 Robohand assistive device, first made available for 3D printing globally via Thingiverse
Robohand assistive device, first made available for 3D printing globally via Thingiverse
Figure 1: The Robohand assistive device, a pioneering example of 3D printed prosthetics, made available globally through Thingiverse, showcasing the impact of open-source designs.
A significant percentage of individuals with both congenital and acquired limb loss choose not to use prosthetics, even when devices are accessible [15]. Usage rates for upper-limb prosthetics are reported to range between 37% [16, 17] and 56% [18] among individuals with upper-limb loss. Lower-limb prosthetics, often perceived as more essential, demonstrate higher usage rates, varying from 49% [19] to 95% [20] in research. This disparity is particularly pronounced among children with transverse upper-limb amputations [21], where usage rates fall between 44% and 66% [22, 23, 24].
Several factors contribute to the low usage rates of upper-limb prosthetics, including a lack of aesthetically pleasing designs, device weight, insurance coverage limitations, healthcare access disparities, and high costs [25]. Furthermore, device acceptance is a complex interplay of user, provider, parental, and insurance considerations. The integration of both form and function in prosthetic design has emerged as a crucial factor, aiming to replicate the intricate functionality of the human hand, with its 21 degrees of freedom [2, 26]. Historically, design efforts have heavily focused on achieving a high degree of realism, mimicking the appearance of a natural limb. However, as Graham Pullin argued in his book “Design Meets Disability” [27], prosthetics should transcend mere functional design, embracing a duality where aesthetics and functionality coexist in harmony.
While research on the benefits of improved prosthetic limb aesthetics remains limited [28], studies suggest that individuals with limb differences may experience lower self-esteem and heightened concerns about negative body image perceptions from others [29]. The psychosocial development effects and quality of life aspects for this population are areas of ongoing investigation. Donovan et al. [28] highlighted how prosthetic use can enhance social engagement and confidence in individuals with limb differences, although their study did not specifically address the visual design or appearance of the limbs. Murray [30, 31] approached the issue from the user’s perspective, finding that prosthetic use positively impacted the psychoemotional well-being of wearers. Further research exploring both the functional advantages and the aesthetic dimension of prosthetics and their impact on user psychosocial development is essential for informing improved design strategies.
2. Contemporary Challenges Driving 3D Printing Prosthetic Innovation
3D printing is rapidly becoming an indispensable technology in upper-limb prosthetics, driven by critical issues such as limited and delayed access to conventional prosthetics and, in many regions, outright lack of access. This review focuses on the evolution of 3D printed prosthetics, the populations they serve, and the core challenges that have propelled their development. Following this, we will discuss the necessary steps to integrate these advancements into mainstream medical systems.
2.1. Prosthetic Limb Abandonment: A Persistent Problem
Patient expectations and daily goals for prosthetic devices are significantly shaped by the type of device they receive [32]. Research indicates that the relative importance of factors like comfort varies based on the user’s perception of the device [32]. For instance, a device with enhanced hand articulation might shift user priorities, potentially diminishing the relative importance of comfort compared to functional performance. The promise of greater control creates heightened expectations for robust and reliable performance. Factors contributing to device rejection also vary based on amputation method, gender, and age [25]. Individuals with congenital limb loss are more inclined to reject devices as adults, while women with acquired limb loss show higher rejection rates than their male counterparts [25]. Prosthetic abandonment is a significant issue across all demographics, stemming from diverse factors. In adult populations, sensory feedback, appearance, function, control, comfort, and durability are consistently cited as crucial areas requiring further attention in prosthetic design and acceptance [25].
Biddiss et al. [33], in a comprehensive review of over 200 research articles, reported pediatric rejection rates of 38% for passive devices, 45% for body-powered devices, and 32% for electric devices. For adults, rejection rates were 39% for passive, 26% for body-powered, and 23% for electric devices. Long-term follow-up data for myoelectric devices remains limited [34]. These significant rejection rates highlight the urgent need to explore innovative approaches to enhance user affinity and improve outcomes.
2.2. The Power of Appearance and Aesthetics
Individuals with limb differences can unfortunately face social stigma due to perceived impairments. Prosthetic limbs can play a vital role in mitigating this stigma. Integrating art and design into prosthetic development can further empower users. Goffman’s theory [35] suggests that social stigma can lead individuals with disabilities to adopt compensatory behaviors to conceal their difference. This can manifest in individuals with limb differences attempting to hide their affected limb in social situations or photographs.
Historically, prosthetics for children often consisted of body-powered hooks or passive, skin-toned devices. Even today, passive or body-powered devices with hooks, sometimes covered with aesthetic silicone gloves, remain a common standard of care [25, 32]. Current trends in prosthetics are shifting towards normalization and reducing the stigma users may encounter. Frank [36] has demonstrated that early prosthetic users can experience empowerment through various means. These positive interactions extend beyond social engagement, fostering personal acceptance of their limb difference, a complex and ongoing process [29]. Advancements in materials are making it increasingly feasible to create prosthetics that closely mimic the natural appearance of a limb. Huang et al. [37] proposed LivingSkin™ silicone elastomer gloving material and innovative motors to achieve a more realistic aesthetic without adding excessive weight. While such devices aim for natural appearance, art-inspired designs can provide individuals with disabilities avenues for self-expression and boost self-esteem [38].
Our research team proposes that combining aesthetic design with functional prosthetics, including designs that intentionally deviate from traditional human form, can foster positive social identities and interactions. This hypothesis is a central focus of our ongoing research.
2.3. Function and Control: Key Determinants of Usability
Modern bionic prosthetics employ three primary control methods [39]: (i) Body-powered control via cable extension or contraction, (ii) button press control [40, 41], and (iii) electromyography (EMG) control. Each method offers distinct user experiences with varying degrees of suitability for daily life. Body-powered devices require gross body movements, often from the torso or shoulder, to manipulate a mechanical hand, hook, or fingers. While less intuitive than natural limb control, they offer functional utility beyond mere cosmetic replacement, addressing specific tasks users encounter daily. Prosthetic selection is typically guided by a patient’s individual needs, experiences, and functional requirements [42]. However, children’s participation in this selection process is often limited. Longitudinal studies comparing outcomes for children fitted with prosthetics versus those without are still lacking [43].
Body-powered devices are more frequently prescribed in the United States and are often considered more robust than myoelectric devices [25, 32, 34]. Body-powered systems provide users with physical sensation feedback, while myoelectric devices primarily offer visual feedback [44]. Due to this and other challenges related to robustness, training complexity, and technical limitations like system weight [25, 32], many professionals and users express a preference for body-powered devices. Control schemes utilizing skin movement or button presses necessitate using another part of the body for control, potentially leading to unintended activations and a less satisfactory user experience.
Electromyography (EMG) stands out as a promising control method, measuring the electrical potential generated by muscle contractions [45]. EMG offers numerous advantages, including a small form factor, reliability, and stability. An EMG sensor equipped with amplification and rectification circuits to condition the signal and integrated filters to remove noise can capture a user’s intended muscle contractions. This filtered signal correlates with the intensity of muscle contraction, which can be used to control the electromechanical hand’s functions. Many prosthetic systems utilize multiple sensors placed on various muscle groups to capture a set of signals for engagement, calibrating these signals to correspond to different organic limb motions [46, 47].
3. A Paradigm Shift in Prosthetic Limb Design: 3D Printing and Open Source
The advent of digital platforms for sharing 3D design models online has fostered a thriving global maker community. A carpentry accident in 2011 sparked a global collaborative effort to restore dexterity for a carpenter, Richard Van As, who lost several fingers [48]. Van As collaborated with Ivan Owen, a mechanical special effects artist. This partnership resulted in the world’s first 3D-printed upper-extremity prosthetic device in 2012. Crucially, the designs were made available in an open-source format, allowing the global maker community to reproduce and refine them. This body-powered device utilized wrist flexion of the residual limb to trigger uniform contraction of the fingers, as illustrated in Figure 1.
3.1. The Rise of 3D Printed Prosthetic Arms and the Maker Movement
The open availability of designs pioneered by Robohand and Ivan Owen had a transformative global impact on the potential applications of accessibility technologies. Their success inspired researchers and maker enthusiasts worldwide to replicate and expand upon their work. Recognizing the effectiveness of collaborative design and production, numerous maker communities and non-profit organizations emerged to facilitate local access, including e-NABLE (http://enablingthefuture.org/), Enable Community Foundation (http://next2.e-nable.me/), Robohand (http://robobeast.co.za/rich-van-as/), and Limbitless Solutions (https://limbitless-solutions.org/). These groups encompass both independent home-based designers and research teams at universities such as Rochester Institute of Technology (RIT), Creighton University, University of Central Florida (UCF), and the University of Washington at Bothell. Additive manufacturing techniques employed range from affordable home-built kit 3D printers to advanced industrial-grade machines. While much of the initial focus was on body-powered devices, some groups have pushed research into electromyographically actuated devices to address more extensive limb loss, incorporating biosensors and electromechanical motors [49].
Custom sizing, achieved through volumetric scaling or precise parametric adjustments tailored to the individual user, enabled rapid production and iterative design. The versatility of 3D printing, allowing for a wide range of filament colors, meant the same base model could be produced in user-specified color schemes, enhancing user engagement and personalization. In 2014, the “Prosthetists Meet 3D Printers” conference at Johns Hopkins Hospital convened the maker community with medical professionals, including surgeons, prosthetists, and therapists, to explore the potential of 3D printing to improve access and quality of care [50]. This landmark conference and the e-NABLE web platform were organized by a team including Jen Owen and Jon Schull, bringing together a diverse group of individuals with limb differences, designers, and medical experts.
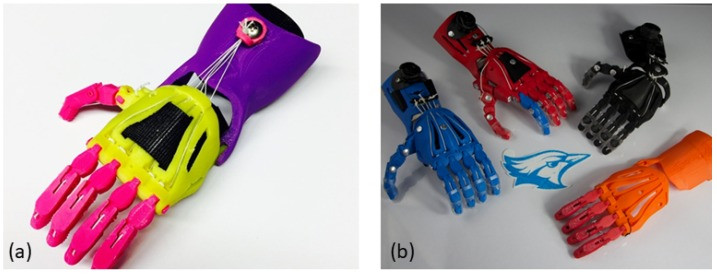
Collaborative design efforts, often leveraging cloud-based real-time design software like Autodesk Fusion 360, facilitated group support and accelerated advancements in functionality, robustness, and user-driven feedback integration. The e-NABLE network made significant design improvements openly available through the Thingiverse.com website, with attribution. Design schematics and example images of printed and assembled parts, such as the Raptor Reloaded hand (https://www.thingiverse.com/thing:476403), shown in Figure 2, became readily accessible. These open-source, customizable designs and the increasing availability of 3D printers in schools, libraries, and homes [51, 52] have dramatically improved prosthetic accessibility for children worldwide.
Figure 2: The Raptor Reloaded hand, a popular open-source 3D printed prosthetic design by e-NABLE, downloadable via Thingiverse, illustrating the accessibility and collaborative nature of 3D printed prosthetic development.
This global collaboration has significantly accelerated the prototyping phase in prosthetic design. A visual representation of the design evolution and the growth of global chapters within the e-NABLE network is available at https://e-NABLE.org, with a comprehensive visualization at https://kumu.io/jonschull/devices.
As the maker movement expanded, integration with university research environments increased. Research groups began focusing on standardizing production methodologies and establishing best practices through data-driven analytics. The work of Jorge M. Zuniga, initially at Creighton University and now at the University of Nebraska, exemplifies this trend. His research [53, 54, 55] has advanced the field of additive manufacturing in biomedical research and its translation to clinical applications. The Cyborg Beast hand, a wrist-powered design developed by Zuniga’s team, built upon earlier work and improved integration and assembly, gaining significant adoption among children with limb differences (Figure 3).
 The Cyborg Beast by Creighton University’s Jorge M. Zuniga and available on Thingiverse
The Cyborg Beast by Creighton University’s Jorge M. Zuniga and available on Thingiverse
Figure 3: The Cyborg Beast, a robust and widely adopted 3D printed prosthetic hand designed by Jorge M. Zuniga at Creighton University, available on Thingiverse, demonstrating the power of academic contributions to open-source prosthetic designs.
Jon Schull, a founder and key figure in the e-NABLE movement, and his research team at RIT made substantial contributions, including new body-powered forearms and hands actuated by elbow or wrist movement. These advancements have facilitated the integration of project-based learning in education [56], utilizing 3D printers and global design networks [57].
3.2. Cooperative Expression: User-Centric Aesthetic Customization
3D printing’s design flexibility enables a high degree of device customization. As the collaborative network of developers expanded, user-driven design became increasingly important. To enhance user affinity for bionic devices, end-user participation has become a priority. Our research team has applied a methodology called “cooperative expression” to prosthetic design, rooted in participatory design principles and strategies like cooperative inquiry.
Participatory design, a research field characterized by diverse methodologies, investigates the crucial role of direct user involvement with designers [58]. Initially applied to computer systems in workplace settings, it is now effectively used to learn from children’s perspectives in developing low-tech design prototypes [59]. Cooperative inquiry, a specific brainstorming method within participatory design, emphasizes collaborative exploration [59, 60]. Druin et al. [59] identified three key dimensions to consider when children are design partners: (i) the child’s relationship with participating adults, (ii) their relationship with the technology, and (iii) the goals of the inquiry. Cooperative inquiry, when applied to technology development, offers flexible frameworks. Foss et al. [61, 62, 63] used this technique to study the role of children with special learning needs and adults as design partners in software development, empowering children to personalize their experiences [62, 63]. Their study using cooperative inquiry reported increased emotional engagement in children, suggesting greater project ownership [62].
Our research team is applying a modified participatory design approach, “cooperative expression,” to the aesthetic customization of 3D-printed bionic limbs to enhance user affinity. This approach actively involves recipients in artistically customizing interchangeable sleeves through an interactive website. Users can compare, select, and personalize various 3D designs, customizing colors and effects. Artists contribute by creating initial aesthetic frameworks, such as color palettes and customizable zones, to guide user exploration and minimize choice overload while encouraging exploration beyond typical preferences.
This unique customization process, outlined in Figure 4, integrates the end-user throughout the design journey. While structural and mechatronic components are standardized, digital designers create 3D artistic shells. An interactive web portal empowers users to customize colors, effects, and regions of the sleeve, providing a visual preview of the final design. Artistic modifications may be incorporated based on user portal interactions to optimize the human-machine interface. Production involves an interdisciplinary process: 3D printing, surface preparation and priming, automotive finishing techniques, and artistic painting. Artists interpret user-selected colors and effects from the portal, enhancing the visual impact. The complete system undergoes validation and fitting. This system ensures active user involvement before production and fitting, fostering an emotional connection to the limb early in the process (Figure 5).
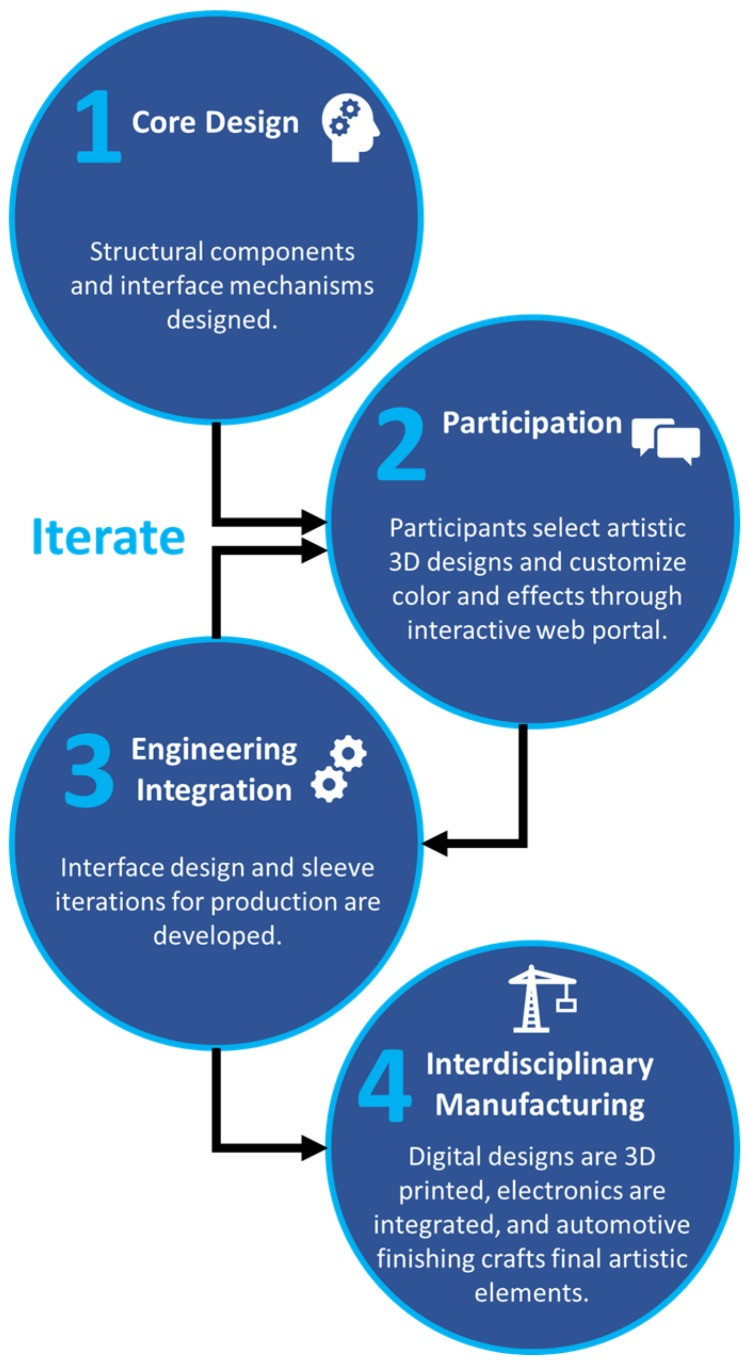 Overview of design process and methodology from design generation, user participation, and interdisciplinary manufacturing
Overview of design process and methodology from design generation, user participation, and interdisciplinary manufacturing
Figure 4: The cooperative expression design process, highlighting the user-centered approach from initial design generation to final interdisciplinary manufacturing, empowering users in the aesthetic creation of their 3D printed prosthetics.
Figure 5: User-driven customization in action: An interactive web interface allowing children to personalize color and effect regions for their prosthetic sleeve (left), demonstrating how user choices are translated into the final artistic design with input from the art and production teams (right). Sleeve design collaboration with Riot Games.
The design process includes “empowerment classes” of interchangeable aesthetic sleeves: Warrior, Shadow, Ethereal, and Serenity. These classes represent distinct personalities linked to emotional affinities. Artists create inspired 3D models aligned with these personalities, and external artists, including character designers, contribute to the design catalog. Examples of these classes are shown in Figure 6. This variety and interchangeability offer children greater expressive freedom, potentially enhancing device affinity, reducing social stigma, and promoting long-term engagement, ultimately improving user performance. Future research will evaluate the impact of this approach on psychosocial development and stigma reduction.
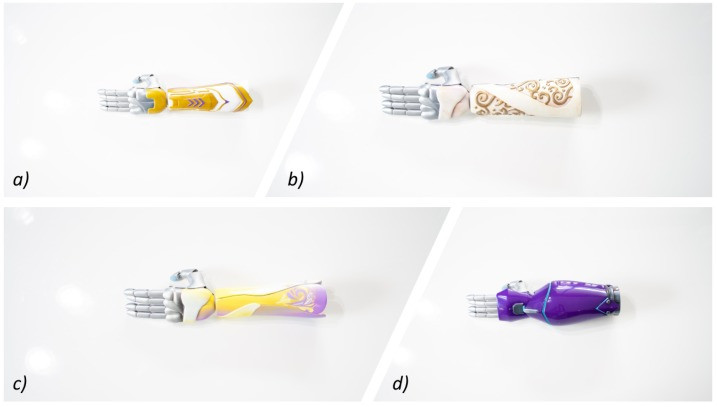 3D-printed electromyographic actuated limb device with interchangeable artistic covers from Limbitless Solutions at the University of Central Florida
3D-printed electromyographic actuated limb device with interchangeable artistic covers from Limbitless Solutions at the University of Central Florida
Figure 6: Empowerment classes of 3D printed prosthetic sleeves developed by Limbitless Solutions, showcasing the artistic diversity and personalization options: (a) Warrior class, (b) Ethereal class, (c) Serenity class, and (d) Shadow class.
3.3. Functionality Enhanced: Electromyography and Simplified Control
Antfolk et al. [44] demonstrated that a 16-sensor EMG system could predict user control intentions with 86% accuracy after a two-day training period in a transradial amputee. The system learned to interpret the user’s EMG input based on movements performed similar to pre-amputation motions [44]. However, increased complexity arises from mapping multiple EMG inputs to multiple computer-controlled outputs. Each additional monitored region requires intentional actuation of corresponding muscle groups, sometimes simultaneously [64]. This complexity can be overwhelming for children and has been linked to device rejection [33].
Our 3D-printed prosthesis utilizes a single EMG measurement, simplifying daily calibration and use. On-board signal processing correlates muscle contraction intensity or the number of contractions within a time period to actuate different hand gestures, including individual finger movements. Addressing limitations of current EMG devices is an opportunity to improve both device design and training methodologies.
3.4. Gamification and Training: Making Prosthetic Control Intuitive
Single-surface EMG providing multi-gesture control allows users to control their prosthesis through contraction intensity and patterns. To address the control complexity, a custom video game-based training system was developed to provide a risk-free learning environment. The game system captures filtered EMG input and routes it to the computer, interpreting it as a multifunction controller or analog input. Training systems incorporating mechanics similar to active arm control, such as punching or slapping with an EMG controller, have shown improved usability scores [65].
Our research team’s latest game for prosthetic arm training, “Magical Savior of Friends” (MSOF), immerses the player in a ‘Mario-style’ side-scrolling adventure. Players control a magical character capable of executing superpower attacks and defenses based on muscle contraction amplitude. After a thresholding calibration sequence, players learn to modulate contraction magnitude, directly influencing the character’s actions. Calibration sets low, mid, and max thresholds, with the low threshold designed to filter out background noise. These calibrated gestures trigger distinct superpower attacks within the game.
While designed to be engaging and fun, MSOF provides meaningful training in complex multi-gesture hand control through simulation. Preliminary results are promising, showing significant improvements in contraction accuracy after just one hour of gameplay [66]. Gamifying the training process offers numerous opportunities for safe failure and feedback in a low-pressure environment. Multiple studies underscore the critical role of feedback in improving myoelectric prosthesis control [33, 44]. Simulation, disguised as a game, effectively facilitates practice and training for prosthesis users. Future work aims to expand this approach, offering prosthesis users access to games they might otherwise be unable to play due to dexterity limitations or interface challenges.
3.5. Comfort and Durability: Addressing Practical Considerations
3D printing, like all manufacturing processes, has advantages and limitations. Its promise of personalized medicine and rapid prototyping is well-demonstrated in clinical settings [67]. While 3D printing is valuable for pre-surgical planning using representative models, concerns about the safety and reliability of 3D-printed parts exist [68]. Professionals utilizing material properties for design optimization must consider the manufacturing process’s impact. Testing of additive manufactured ABS plastic reveals variable mechanical properties depending on print orientation, with strengths ranging from 10% to 73% of injection-molded samples [69, 70]. While layer printing methods influence deviations from material standards, optimization strategies can enhance reliability and performance predictability [69, 71]. Consistent standards and best practices are crucial for reliable 3D-printed components in medical applications. FDA guidelines provide recommendations for workflow and part tracking [71], but deeper understanding of part vulnerability principles can proactively minimize risks. Designed with realistic loading expectations and manufacturing considerations, additive manufacturing can produce stable, resilient parts, reducing system weight and manufacturing costs [72].
4. Navigating the Regulatory Framework for 3D Printed Prosthetics
While extensive research is dedicated to advancing novel manufacturing techniques in prosthetics, reviews of current studies highlight areas needing further development [73, 74]. An independent review [73] of 314 studies found a prevalence of case studies over randomized controlled trials. Areas needing improvement included study power, statistical rigor, reliable outcome measures, and recruitment clarity. The review [73] emphasized the need for robust efficacy and effectiveness evaluations to provide healthcare professionals with evidence-based information for informed patient care decisions.
To advance the field and quantify the impact of our 3D-printed electromyographically actuated multi-gesture arms, a novel clinical trial is underway through a collaboration between Oregon Health & Science University and the University of Central Florida. This study, deemed non-significant-risk, involves twenty participants aged 6 to 17 in a one-year trial with four assessments. Assessments are twofold: quality of life impact (using the Children’s Hand-Use Experience Questionnaire (CHEQ) and PedsQL) and myoelectric control (using the Assessment of Capacity for Myoelectric Control (ACMC)).
CHEQ, a four-category rating scale for children aged 6-18 (available at www.cheq.se [75]), assesses functionality and limitations. Its nested question structure begins with “Is this something you usually do independently?” with options: ‘yes’, ‘no’, ‘I get help/avoid doing it’, or ‘not applicable’. “Yes” responses trigger a second question: “Do you use one hand or both hands together?”, with options: ‘one hand’, ‘both hands’, ‘with the involved hand supporting but not holding’, or ‘both hands, with the involved hand holding the object’. This assessment [75] provides a reliable baseline for understanding the impact of limb difference on daily life.
PedsQL, a validated 23-question survey for parents and children, assesses health-related quality of life over the past month. Published results are available for general populations. PedsQL scoring translates responses (“never”, “almost never”, “sometimes”, “often”, “almost always”) into scores (0%, 25%, 50%, 75%, 100%) across four core scales: Physical Health, Emotional Functioning, Social Functioning, and School Functioning.
ACMC [76, 77], a Rasch rating scale, measures changes in prosthetic arm function using 30 items evaluating gripping, holding, releasing, and inter-limb coordination. Tasks include daily chores like meal preparation and table setting, and leisure activities such as LEGO assembly [76, 77]. Occupational therapists assess performance, and participant feedback is documented. Study findings will inform design and methodology improvements.
5. Conclusion: 3D Printing Prosthetics – A Future of Accessible and Personalized Care
The future of 3D printing in prosthetics, coupled with collaborative design, is promising. Rapid iteration and user-centered designs are fostering greater user affinity. However, robust clinical assessments are still needed [73, 74]. Our novel clinical assessment of 3D-printed EMG bionic limbs, using well-defined outcome metrics, aims to contribute to the field and assess readiness for wider adoption. Continued validation of design and performance will improve technology and design method translation. The user-centric design process and significant cost reductions offered by 3D printing have the potential to revolutionize the accessibility of functional prosthetics, particularly for pediatric patients, paving the way for a more inclusive and personalized future of prosthetic care.
Acknowledgments
The authors express their gratitude to the dedicated members of the Limbitless Solutions team for their unwavering support throughout this project’s development. We extend our sincere appreciation to Riot Games and 343 Industries for their invaluable contributions of additional designs to the sleeve catalog.
Author Contributions
Conceptualization: A.M., P.S., A.C.; Original draft preparation: A.M., P.S. (with support from J.S., M.D., D.C., A.K., I.W., A.C.); Review and editing: all authors.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no personal conflict of interest but acknowledge that Limbitless Solutions has received support from Stratasys, a 3D printer manufacturer.
References
[1] … (References as in the original article)
[2] …
[3] …
[4] …
[5] …
[6] …
[7] …
[8] …
[9] …
[10] …
[11] …
[12] …
[13] …
[14] …
[15] …
[16] …
[17] …
[18] …
[19] …
[20] …
[21] …
[22] …
[23] …
[24] …
[25] …
[26] …
[27] …
[28] …
[29] …
[30] …
[31] …
[32] …
[33] …
[34] …
[35] …
[36] …
[37] …
[38] …
[39] …
[40] …
[41] …
[42] …
[43] …
[44] …
[45] …
[46] …
[47] …
[48] …
[49] …
[50] …
[51] …
[52] …
[53] …
[54] …
[55] …
[56] …
[57] …
[58] …
[59] …
[60] …
[61] …
[62] …
[63] …
[64] …
[65] …
[66] …
[67] …
[68] …
[69] …
[70] …
[71] …
[72] …
[73] …
[74] …
[75] …
[76] …
[77] …
